From Injury to Performance: An ACL Healing Beyond Surgery
Patient profile
Age and gender: 28-year-old male
Occupation – Chartered Accountant
Complaints – Left side ACL tear
HISTORY:
Present history
He is a recreational football player. In October 2024, he twisted his left knee while playing football. After returning home, he applied ice for 2 days but got no relief. It was swollen and painful.
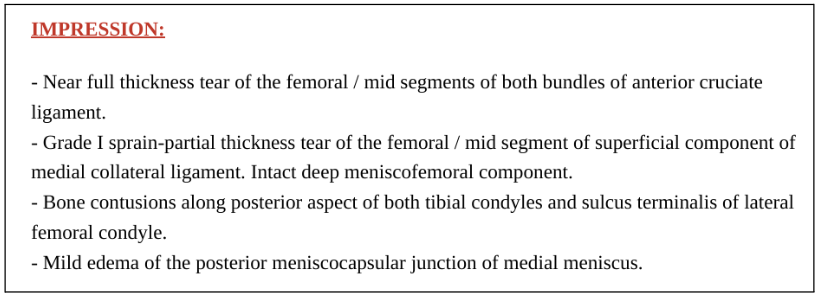
Later, after 2 days, he consulted with a doctor and took an MRI, which showed a near full-thickness ACL tear and grade 1 sprain in the medial collateral ligament. From the time of injury till now, he has felt instability in his left knee.
Past History:
In March 2017, he was in college, studying to be a chartered accountant. While playing football, he twisted his Right knee. Immediately, he had swelling and pain. He thought it might be a minor injury, so he took some rest and waited for almost a month to resolve it.
Later, he started doing some running and felt severe pain in his knee. Then, he consulted with a doctor who suggested an MRI, which showed a full ACL tear.
From May 2017 to June 2019, he consulted many physios and underwent treatment. Yet, proper rehabilitation was not done due to his inconsistency and lack of structured physiotherapy planning. During that period, he experienced 15-17 episodes of buckling.
In July 2019, he underwent surgery and began physiotherapy, which he continued for 4-5 months. Unfortunately, due to the COVID-19 pandemic, proper rehabilitation was not done, and RTS (Return to Sport) testing was not conducted. Later, he gradually resumed playing at home and was given gradual exposure to the game. By 2021, he had returned to playing on the field and had begun consistent gym training for 3 days/week.
Beliefs and expectations:
Since he had experience with a similar injury on the opposite side and underwent surgery, he felt that this injury was not serious enough to undergo surgery immediately. So, he thought of managing it without surgery, so he came to us for the non-surgical management of an ACL tear. He wants to prevent further injury, get fit, and play again.
Sleep – Slightly disturbed. He is trying to work on it.
Stress – He is a little stressed because of another injury.
Physical activity status – Before the injury, he played 2–3 times a week and worked out three times a week. After the injury, he started doing exercises on his own as he had previous treatment experience.
Goal/ Objective of his consultation with us:
- He wants to go for non-surgical rehabilitation.
- His motive is to play football again recreationally.
PAIN ANALYSIS:
Mild discomfort in the left knee while loading.
Fear of movement analysis
Partially positive because of past injury history. But he has a good attitude towards movements.
An important aspect of the history that we discovered is:
- No proper and consistent rehab, and RTS testing were done for the previous injury.
PHYSICAL EXAMINATION:
1. Observational findings
- Good muscular physique
- Muscle mass is very slightly reduced on the left lower limb.
- Mild swelling present on left knee, medial side.
2. Muscle mass circumference
| All measurements were taken from the proximal border of the patella | Right (cm) | Left (cm) |
|---|---|---|
| Above 5 cm | 17.2 | 16.3 |
| Above 10 cm | 21 | 20 |
| Above 15 cm | 19 | 18.5 |
3. Mobility/ROM screening:
| Test | Right side | Left side |
|---|---|---|
| Hip ER ( FABER) (distance from the floor) | 6.5inch | 8 inch |
| Ankle DF (5-inch ankle mobility test) (distance from the wall) | 2.2 inch | 3.1 inch |
| Knee flexion | 117° | 125° |
| Terminal Knee extension | 0° | 0° |
Strength test:
| Movements | Right | Left | Limb symmetry index |
|---|---|---|---|
| Single-leg sit-to-stand with body weight | 32+3 | 27+2 | 84% |
| Single-leg glute bridging with body weight | 39sec | 30sec | 76% |
| Side plank leg lift with body weight | 44sec | 32sec | 72% |
| Single-leg hamstring bridging with body weight | 25 | 19 | 76% |
| Single leg calf raise 16kg KB) | 22 | 24 | 109% |
| Hip flexor strength | 25 | 21 | 84% |
Note: This person has already undergone ACLR in the right leg, but proper RTS tests were not done. So, comparing the limb symmetrical index between the currently injured leg and the non-painful (previously injured) leg is not accurate and reliable. Tests are done to help with clinical correlation.
Single leg standing with eyes open, eyes closed > 90% similar to right side.
Standing hop performance > 90% similar to the right side.
Special test:
- Lachman test: it feels like +ve, but no significant translation was observed.
- Mc Murray test: -ve
- Valgus test: -ve
INVESTIGATION:
MRI – Full ACL tear + Grade 1 tear/sprain in MCL
DIAGNOSIS:
1) What is the patient’s perception of non-surgical rehab?
He had experienced an ACL tear on the opposite side and underwent ACLR. This time, he feels that the injury isn’t very severe, so he opted for non-surgical rehabilitation.
Psychosocial factor analysis
| Cognitive | Not affected much |
| Affective | Not affected much |
| Social | Not affected much |
2) Clear explanation for decision making:
During consultation, there was no sign of significant swelling or pain. Based on physical examination, we found that his left side muscle mass and strength are slightly reduced than the right side, and the severity of the injury is not so severe. It is not clinically correlated with the MRI reports.
We went through a 24-point decision-making approach, which was designed in our clinic.
| S.no | 0 | 1 | 2 | Scoring | |
|---|---|---|---|---|---|
| 1 | Pain | Sports activity | Functional activity | Rest | 1 |
| 2 | Swelling | Sports activity | Functional activity | Rest | 0 |
| 3 | ROM Knee flexion | Both good | Any one good | Both active and passive affected | 0 |
| 4 | Terminal knee extension | Both good | Any one good | Both active and passive affected | 0 |
| 5 | Muscle mass | Not affected | Slightly affected | Highly affected | 1 |
| 6 | Muscle strength | S/L squat complete stand | Partial ability to stand | Unable to stand | 1 |
| 7 | Stability and Balance | Relatively the same in both legs | 50% of the unaffected side | >50% of the affected side | 1 |
| 8 | Instability episode | No | 1 | >1 | 2 |
| 9 | Special test | -ve | Partially +ve | +ve | 1 |
| 10 | MRI findings | Good. No significant changes/grade 1 tear or strain | Grade 2 tear | Grade 3 tear | 2 |
| 11 | RTS | Not needed | Recreational | Elite | 1 |
| 12 | Hop performance | Unable | Tried | Doing good | 1 |
| Total | 11/24 | ||||
*Scale is subjective, created based on clinical experience.
Percentage of requiring surgery = Total score/24 x 100 = 11/24 x 100 = 45.83%
If score <50% – Rehab alone, or start with rehab first and then opt for a delayed surgery. (if required)
TREATMENT PLANNING:
Research indicates that returning to play after an ACL injury typically requires approximately 9 months to play professionally. Athletes who resume sports earlier have a 7 times increased risk of reinjury. https://pubmed.ncbi.nlm.nih.gov/27162233/
Initially, plan to go for a three-month rehabilitation program, after which, if required, suggest going for surgery.
The three-month rehabilitation program includes
- Functional strength testing
- Strength training and neuromuscular control training
- Coper’s classification testing
- Return to running the criteria testing
- Return to sports criteria testing
Treatment approach:
The first few weeks focus on individual unilateral muscle strengthening with neuromuscular control and balance training. It helps in
- Reducing muscle imbalances
- Improving stability and balance
- Reducing Intralimb and interlimb compensatory movements
- Reducing the chance of re-injury
Later, it can progress to bilateral strengthening with progressive loading, cardio, mild agility, and plyometrics with running.
Coper’s classification:
| Screening test | Coper classification threshold |
|---|---|
| Timed 6m hop, symmetry | >=80% |
| Knee outcome survey | >=80% |
| Global rating scale score | >=60% |
| No. of giveaway episodes | <=1 |
Coper
- Can return to high-level activities without instability.
- Exhibit good neuromuscular control and knee function.
- Typically perform well in functional hop tests and knee stability assessments
If the patient cannot meet the coper threshold, he should go for the surgery.
If the patient can meet the coper threshold, he is eligible to go for return to running testing and then return to sports. Check if there is:
- No pain
- No swelling
- Full flexion
- Full extension
- LSI >85%
Once he achieves these, he’ll be eligible for RTR, which demands:
- S/L hop test [ >95% ]
- Triple hop test [ >95% ]
- Triple crossover hop test [ >95% ]
- Side hop test [ >95% ]
- S/L squat =>22 reps in both limbs
- Balance – Star Excursion Balance Test >95% compared to opposite limb
- S/L press with 1.8 x Body weight
- Squat with 1.8 x Body weight
After clearing RTR criteria, treatment focuses on Plyometrics and agility training with conditioning.
Later, we can test the RTS criteria.
After passing this test, the patient can return to practice in the field and then participate in non-competitive football games.
| Phase – I 1–3 months | Strength and Neuromuscular control | |
|---|---|---|
| Target | Strength | Mobility with Individual strengthening |
| Neuromuscular control | Isometric progression along with Isotonic loading, balance coordination, and cardio exercises. | |
| Exercises (example) | Strength | Supine scorpion, ATG, Hip flexor, kneeling adductor, Hamstring stretching, Quad and glute isometric strengthening. |
| Neuromuscular control | Quad extension, hamstring curl, easy body weight exercises, and progressed. | |
| Goal | Regain full knee ROM Eliminating swelling Regain muscle strength S/L squat with good tech and alignment | |
| Outcome measure | S/L bridges [>85% ] Calf raises [ >85% ] Side plank [ >85% ] Single leg squat [ >85% ] Balance eyes open [43 sec] and eyes closed [ 9 sec] S/L press 1.5x BW Squat 1RM – 1.5x of BW | |
| Phase – II 3–5 months | Running, agility, and landing |
|---|---|
| Target | Progressively increase volume in isotonic loading, incorporating some decelerating force absorption activities along with cardio and coordination exercises, and progress. |
| Exercises (examples) | Forward step up, Goblet squats, KB lift, Hip thrust, shin and calf raises, etc., with some fast walking and gait re-education drills, ladder exercises, side shuffle, jumping, etc. |
| Goal | Attain excellent hoping performance Regain full strength and balance Progress Agility Programme |
| Outcome measure (RTR criteria) | S/L hop test [>95% ] Triple hop test [>95% ] Triple crossover hop test [>95% ] Side hop test [>95% ] S/L squat =>22 reps Balance – star excursion test >95% compared to the other limb S/L press 1.8x of BW Squat 1.8x of BW |
| Phase – III 5–9 months | Return to sports criteria |
|---|---|
| Outcome measure | Clinical examination IKDC subjective knee evaluation and ACL RSI Tampa scale of kinesophobia Functional testing Assessment of general fitness Functional testing in a fatigued state |
| Phase – IV | Recurrent Injury Prevention |
|---|---|
| Prevention of re-injury | Maximum exposure to the game with warm-ups, sports-specific, and strength and conditioning |
| Goal | Plyo, strengthening exercises Warm-up program, at least 10 minutes before play |
| Outcome measure | Sports matric program The 11+ warmup The PEEP program The knee programme, Netball Australia. The Footy, the first programme, AFL. |
Principles of ACL Rehab:
- Follow fundamentals – Basic to advanced
- Don’t forget to add cardio
- Consider the neuro-recognitive aspect of rehab
- Don’t rush or overcomplicate- stick to basics
- Train to the non-injured side too
- Give adequate time to RTR
- Psychological support if needed
| Phase- II 3–5 months | Running, agility, and landing |
|---|---|
| Target | Progressively increase volume in isotonic loading, incorporating some decelerating force absorption activities along with cardio and coordination exercises, and progress. |
| Exercises (examples) | Forward step up, Goblet squats, KB lift, Hip thrust, shin and calf raises, etc., with some fast walking and gait re-education drills, ladder exercises, side shuffle, jumping, etc. |
| Goal | Attain excellent hoping performance Regain full strength and balance Progress Agility Programme |
| Outcome measure (RTR criteria) | S/L hop test [>95% ] Triple hop test [>95% ] Triple crossover hop test [>95% ] Side hop test [>95% ] S/L squat =>22 reps Balance – star excursion test >95% compared to the other limb S/L press 1.8x of BW Squat 1.8x of BW |