Contents
- 1 SLAP Tear Simplified
One-stop resource: from Pain to performance
- 1.1 What exactly is a SLAP Tear?
- 1.2 How Do SLAP Tears Happen?
- 1.3 What are all the symptoms experienced by the patient?
- 1.4 Diagnosing SLAP Tears:
- 1.5 What is the best treatment approach?
- 1.6 Rehabilitation
- 1.7 Reference
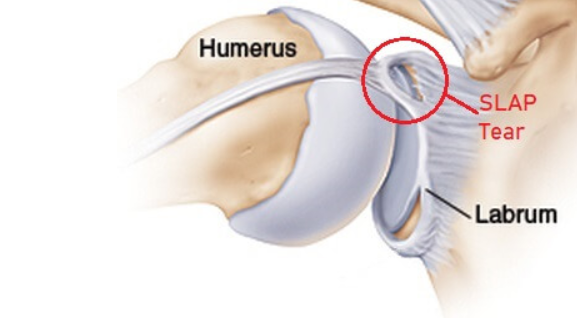
How Do SLAP Tears Happen?
The underlying cause is often multifactorial – shoulder anatomy, mechanics, workload, and fatigue all play a role. But the injury may be due to
Acute Traumatic Injuries
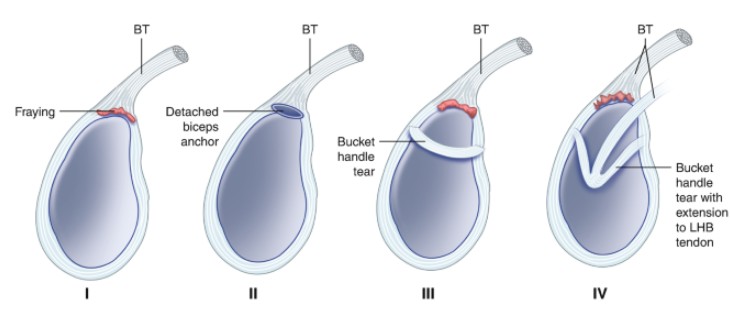
Trauma can tear the labrum in one of three ways:
- Compression-type injuries: Falling on an outstretched arm (FOOSH) with your arm in various positions of abduction.

2. Traction-type injuries: A sudden jerking pull, such as water skiing, losing grip on a heavy object, or grabbing something overhead to stop a fall.

O’Brien’s test.

Biceps load test I

Biceps Load Test II

Then, how to diagnose?
A comprehensive approach consists of history, physical examination, a cluster of special tests, and MRA imaging for greater accuracy in diagnosing SLAP tears.
Differential diagnosis
Differential diagnosis analysis is crucial.
Other conditions that mimic SLAP tear symptoms include:
- Rotator cuff tendinopathy
- Biceps strain
- Subscapularis strain
- Pectoralis major strain
- Internal impingement
- Even referred pain from the cervical spine
Does it really matter, and will it change the treatment plan? I think it may be a little, but overall, it will remain a pretty similar treatment approach to other similar pathologies.
What are the clinical features of the above conditions?
1. Biceps Strain
- pain and tenderness over the bicipital groove/arm
- pain with supination/flexion
- Speed’s test +ve
2. Pec Major Strain
- Pain in Anterior chest/axilla
- Weakness in adduction & IR
- Pain in resisted horizontal adduction
- History of Bench press injury
3. Subscapularis Strain
- Pain over Anterior shoulder
- Weakness in internal rotation
- Lift-off test +ve
- Pain reaching behind the back
4. Rotator Cuff Tendinopathy
- Pain over the Lateral shoulder/deltoid
- Night pain
- Hawkins-Kennedy test +ve
5. Internal Impingement
- Pain in the Posterior shoulder
- Pain in late cocking
- 90/90 ER test +ve
- Overhead athletes are more common (especially those who have GIRD)
What is the best treatment approach?
Nonoperative treatment of SLAP tears in athletes can be successful, especially in the subset of patients who can complete their rehabilitation program before attempting a return to play.
Non-Surgical Management
- What conservative treatments are available? Options include rest, physical therapy, injections (such as lidocaine or PRP), and non-steroidal anti-inflammatory drugs (NSAIDs). But do these conservative treatments really work? What does the research say about their effectiveness?
- Most clinicians recommend 3-6 months of rehabilitation before considering surgery. Why? Because even if imaging confirms a tear, surgery doesn’t always guarantee a successful return to play, especially for high-level overhead athletes.
- Research shows that some athletes who fail their first rehab attempt may succeed with a second, if the program is well-structured and progressive.
- Research shows that the average time to return to play after non-surgical management varies from 5.2 months to 5.7 months, with an average session required for successful rehabilitation is 20 sessions (8-18)
Surgical management
- A study by Frantz et al., 2020 and Recker et al 2022 shows that Biceps tenodesis offers encouraging functional outcomes and RTS rates, particularly in recreational athletes, than Labral repair.
- But another study by Schrøder CP et al., 2017 shows that neither labral repair nor biceps tenodesis had any significant clinical benefit over sham surgery for patients with SLAP II lesions.
- Thus, Surgery is considered when:
- Non-operative care fails
- Symptoms persist and significantly limit performance
- Imaging + clinical exam strongly suggest an unstable tear
- Procedures vary based on age, sport, and surgeon preference (labral repair, biceps tenodesis, debridement, etc.).
- But surgery is not the end. A 9-12 month rehab program is still needed for full recovery.
Rehabilitation
Rehabilitation isn’t just about regaining function. For some individuals, it makes them do their daily activities. For some individuals, it helps them get back to their work. For athletes, it’s about preparing them to return stronger and more resilient to the sport.
Phase 1: Restore Full, Pain-Free ROM and Strength
- Use the uninjured shoulder as a reference (ROM, Strength), but remember that Overhead athletes often have natural side-to-side differences.
- Focus not only on the shoulder, but also periscapular muscles, trunk, pelvis, and lower body conditioning.
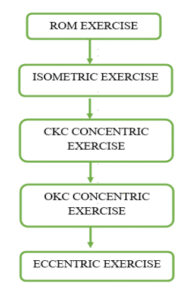
Components of resistance training (11,12,13)
- Isometric and ROM exercise – Activates RC muscles and scapular stabilisers without stressing the biceps anchor or labrum.
- Closed kinetic chain (CKC) concentric exercise – provides co-contraction and joint compression, introduces low shear forces to the shoulder.
- Open kinetic chain (OKC) concentric exercise – Introduces high shear force. Allows us to strengthen the shoulder muscles in a more functional range
- Eccentric exercise – Builds tendon/ labral tolerance and prepares for overhead and throwing demands.
- Focus on cardiovascular fitness as well.
- At the end of this phase, ensure that adequate progress is made in terms of strength, ROM, and that it is measured objectively throughout the rehabilitation, preferably with a hand-held dynamometer ( can also use maximum RM strength testing ) and an inclinometer/ goniometer.
Phase 2: Introduce Plyometrics and Power Strength (Build on strength with explosive exercises)
- 2–3 sessions per week, with 48 hours rest in between.
- Mix plyometric and resistance training.
Components of Plyometric Exercise

- Force absorption (e.g Med ball catch, catching a ball in an open chain)

- Force creation (e.g Pendlay rows, Bench throws, Ball throws for distance)

- Stretch shortening cycle phase (e.g Plyometric push up, Push press, Med ball catch and throws)

- Maximal demand phase (e.g Shoulder hops, Push jerks, Reactive ball catches, Return to sport-specific throwing)
Phase 3: Throwing Programme
- Gradual, stepwise return to throwing/serving/spiking.
- The programme should be performed every other day to allow one day of recovery and evaluation.
Phase 4: Return to Sport Testing
- There’s no gold-standard RTS test yet, but clinicians simulate worst-case demands of the sport (e.g., clinching, blocking, throwing under fatigue).
- We can utilise RTS tests for the shoulder recommended in a paper by Schwank, Ariane et al., 2022.
Sport-Specific Tests Recommended by the Delphi Group for Overhead (With or Without Throwing) Athletes and Collision-Sport Athletes
| Performance Test | ROM/Strength Test | Kinetic Chain | Sport-Specific Test Example |
|---|---|---|---|
| CKCUEST | 90°/90° concentric/eccentric rotator cuff testing | Push-up test: assessing for ability, quality of movement, control, and endurance | Number of pain-free throws/serves at or above previous speed |
| PSET | Isometric rotation strength ER/IR at 90°/0° | Side plank endurance | Throwing at full speed |
| Shoulder Endurance Test (SET) (endurance test for ER in ABD/ER, 90°/90°) | Total rotational ROM within 10% of the contralateral side | Plyometric push-up | Visual assessment of the “smoothness” of the throwing technique |
| The Athletic Shoulder Test (ASH-Test) | ER force measured with HHD in prone at 90°/90° and 90°/0° | Single-leg squat test | Wrestling drills |
| Y Balance Test for the upper and lower extremities | ER/IR ratio: sport-specific numbers apply | Thoracic spine rotation | Tackle replication (eg, for American football or rugby) |
| Seated medicine-ball throw | IR/ER ratio at 90°/90° in sitting (break test, HHD) | Bench press | |
| Ball abduction-ER test | |||
| IR/ER ratio in sitting at 90° of abduction and neutral rotation | Upper-limb rotation test | ||
| Ball taps on the wall test | … | … | … |
| Prone ball-drop test | … | … | … |
- Shared decision-making between the athlete, the medical team, and coaches is essential while sending the athlete back to the sport.
- Also, assess the player’s psychological readiness and confidence along with RTS, as it plays an important role in RTS.
Phase 5: Return to Performance
Getting back to competition ≠ , regaining peak performance. True return to form is often achieved only after full competition exposure.
Research shows that the return-to-play rate was 53.7% in all athletes and 52.5% in elite or higher-level athletes. In athletes who were able to complete their nonoperative rehabilitation program, the return-to-play rate was 78% in all athletes and 76.6% in elite or higher-level athletes. The overall rate of return to prior performance was 42.6%, which increased to 72% for those athletes who were able to complete their rehabilitation.
Take-home message
- SLAP tears are common in overhead athletes and often present with vague symptoms like deep shoulder pain, popping, or loss of throwing velocity.
- Diagnosis is challenging- a combination of history, physical exam, special test clusters, and selective imaging gives the best accuracy.
- Non-surgical rehab is the first-line treatment, with structured programs showing higher return-to-play rates than surgery.
- Rehabilitation must be progressive, moving from ROM and strength to plyometrics, throwing, RTS testing, and finally returning to performance.
- Successful return to sport depends not only on physical healing but also on workload management and psychological readiness
Reference
- Steinmetz, Raymond G et al. “Return to play following nonsurgical management of superior labrum anterior-posterior tears: a systematic review.” Journal of shoulder and elbow surgery vol. 31,6 (2022): 1323-1333. doi:10.1016/j.jse.2021.12.022
- Freijomil, Nicholas et al. “THE SUCCESS OF RETURN TO SPORT AFTER SUPERIOR LABRUM ANTERIOR TO POSTERIOR (SLAP) TEARS: A SYSTEMATIC REVIEW AND META-ANALYSIS.” International journal of sports physical therapy vol. 15,5 (2020): 659-670. doi:10.26603/ijspt20200659
- Clark, Richard C et al. “USE of CLINICAL TEST CLUSTERS VERSUS ADVANCED IMAGING STUDIES in the MANAGEMENT of PATIENTS with a SUSPECTED SLAP TEAR.” International journal of sports physical therapy vol. 14,3 (2019): 345-352. doi:10.26603/ijspt20190345
- Michener, Lori A et al. “National Athletic Trainers’ Association Position Statement: Evaluation, Management, and Outcomes of and Return-to-Play Criteria for Overhead Athletes With Superior Labral Anterior-Posterior Injuries.” Journal of athletic training vol. 53,3 (2018): 209-229. doi:10.4085/1062-6050-59-16
- Schrøder CP, Skare Ø, Reikerås O, et alSham surgery versus labral repair or biceps tenodesis for type II SLAP lesions of the shoulder: a three-armed randomised clinical trial. British Journal of Sports Medicine 2017;51:1759-1766.
- Borkar, Tejas. “Recent Trends in Rehabilitation and Return to Sports Criteria Post SLAP Lesion in Overhead Athletes – A Systematic Review.” International Journal of Health Sciences and Research, 2024.
- Schwank, Ariane et al. “2022 Bern Consensus Statement on Shoulder Injury Prevention, Rehabilitation, and Return to Sport for Athletes at All Participation Levels.” The Journal of Orthopaedic and Sports Physical Therapy, vol. 52,1 (2022): 11-28. doi:10.2519/jospt.2022.10952
- LeVasseur, Matthew R et al. “SLAP tears and return to sport and work: current concepts.” Journal of ISAKOS: joint disorders & orthopaedic sports medicine vol. 6,4 (2021): 204-211. doi:10.1136/jisakos-2020-000537
- Mathew, Cristin John, and David Mark Lintner. “Superior Labral Anterior to Posterior Tear Management in Athletes.” The Open Orthopaedics Journal, vol. 12, no. 1, 31 July 2018, pp. 303–13, https://doi.org/10.2174/1874325001812010303.
- Dodson, Christopher C, and David W Altchek. “SLAP lesions: an update on recognition and treatment.” The Journal of Orthopaedic and Sports Physical Therapy, vol. 39,2 (2009): 71-80. doi:10.2519/jospt.2009.2850
- Gaunt, Bryce W et al. “The American Society of Shoulder and Elbow Therapists’ consensus rehabilitation guideline for arthroscopic anterior capsulolabral repair of the shoulder.” The Journal of Orthopaedic and Sports Physical Therapy vol. 40,3 (2010): 155-68. doi:10.2519/jospt.2010.3186
- Wilk, Kevin E et al. “Non-operative rehabilitation for traumatic and atraumatic glenohumeral instability.” North American journal of sports physical therapy: NAJSPT vol. 1,1 (2006): 16-31.
- Popchak, A., Patterson-Lynch, B., Christain, H., & Irrgang, J. (2017). Rehabilitation and return to sports after anterior shoulder stabilisation. Annals Of Joint, 2(10). doi:10.21037/aoj.2017.10.06
- Lansdown, Drew A et al. “Imaging-Based Prevalence of Superior Labral Anterior-Posterior Tears Significantly Increases in the Ageing Shoulder.” Orthopaedic journal of sports medicine vol. 6,9 2325967118797065. 17 Sep. 2018, doi:10.1177/2325967118797065
- Frantz, Travis L et al. “Biceps Tenodesis for Superior Labrum Anterior-Posterior Tear in the Overhead Athlete: A Systematic Review.” The American journal of sports medicine vol. 49,2 (2021): 522-528. doi:10.1177/0363546520921177
- Recker, Andrew J et al. “Biceps Tenodesis Has Greater Expected Value Than Repair for Isolated Type II SLAP Tears: A Meta-analysis and Expected-Value Decision Analysis.” Arthroscopy: the journal of arthroscopic & related surgery: official publication of the Arthroscopy Association of North America and the International Arthroscopy Association vol. 38,10 (2022): 2887-2896.e4. doi:10.1016/j.arthro.2022.05.005
Azarudheen is a passionate physiotherapist and exercise prescriptor with a deeply rooted belief in the transformative power of movement and education. His journey began in 2013 as a first-year physiotherapy student, balancing academics with part-time work to support his ambitions. Early in his career, he sought practical experience and began working at a fitness center, eventually transitioning into roles that expanded his knowledge and skill set in both clinical practice and teaching.
Driven by a relentless curiosity and desire for growth, Azarudheen took on an anatomy tutor position, believing in the value of continuous learning. A pivotal turning point came with his experience in cardiopulmonary rehabilitation at PSG Hospitals, where he worked closely with lung transplant patients. This experience emphasized the life-changing impact of functional movement and patient education, inspiring him to dive deeper into respiratory and cardiovascular physiology.
With strong support and belief in his vision, Azarudheen pursued a Master’s in Exercise and Sports Science at Manipal University—choosing it over conventional MPT programs to focus more on biomechanics, exercise physiology, strength and conditioning, and lifestyle health. His dedication was evident as he spent late nights at the library, worked part-time in gyms and cricket academies, and honed his craft through practical application.
In 2022, despite initial doubts, he opened his first clinic in his hometown—an act of courage and self-belief supported by his family and mentors. Built from the ground up, this clinic marked the start of a new era. Today, Azarudheen leads a growing team of 21 physiotherapists across two thriving clinics in Chennai and Coimbatore. His philosophy centers on patient education, movement optimization, and professional growth, and he continues to evolve both as a clinician and a leader.
Azarudheen’s journey reflects the power of perseverance, vision, and lifelong learning. He is not only a practitioner but also a mentor and advocate for a more thoughtful, movement-centered approach to healthcare.