
Case prepared by: Ameen
Diagnosis of NON-SPECIFIC LOW BACK PAIN
Patient Profile
- Age/Gender: 30-year-old male
- Occupation: IT professional
- Chief Complaint: Bilateral Low back pain with hip and lateral thigh pain (7 months duration)
History
The patient reports a 7-month history of bilateral low back pain radiating to the hips and lateral thighs. Symptoms began gradually after treatment for a sudden unilateral headache. Following the medication, he developed a mild fever and subsequently noticed the onset of low back pain.
He underwent 20 sessions of physiotherapy, but there was no improvement. MRI and CT scans were normal, while blood tests revealed deficiencies in Vitamin D and B12.
Temporary relief (≈50%) was achieved with Siddha treatment, but symptoms recurred. Over the course of his condition, he experienced disturbed sleep, reduced physical activity, and significant weight loss (12–15 kg) due to dietary restrictions. Ayurvedic treatment, combined with rest and massage, also did not provide sustained improvement.
He visited our clinic seeking complete recovery and return to normal function.
Physical activity status:
Physical activity level is poor since the patient reduced activities due to advice from Siddha, Ayurveda, in the past 6 months
Sleep:
Poor due to pain; he sleeps only for 4 hours/day
Stress:
High stress because of recurrent pain and not being able to play with his children
Past medical/surgical history
No relevant history related to his current complaints
Pain Analysis
- Intensity: 7/10
- Onset: Gradual
- Aggravating factor: Standing, walking, sleeping
- Relieving factor: Rest, sitting
- Location: Bilateral Low back, hip and lateral thigh
- Duration: 7 months
- Lifestyle factor impact: High – stopped most ADLs
- Fear of movement analysis: Doctor-induced fear was there.
Psychosocial factor analysis
- Cognitive – He had lots of negative beliefs regarding pain
- Affective – He is affected. Because of the pain, he is not able to play with his child, causing emotional distress.
- Social – Good
Our understanding of patients' problems:
Since the back pain is associated with a systemic illness(fever), it gives an indication of any specific spinal pathology. But the patient’s overall lifestyle shows that his physical activity is poor, psychologically affected and has fear avoidance behaviour, which can be a major contributing factor for pain. So we have to thoroughly assess to confirm whether it is a specific spinal pathology or a non-specific low pain.
Physical examination
Observational findings: Nil
Palpation:
No pain on palpation over the low back, hip and thigh
Mobility screening
- The forward-bending movement quality is good
- Overhead squat is good, no shifts
ROM analysis
There is no significant difference between right and left in HIP, knee and ankle ROM
Stability screening
The break test was done for the lower limb group of muscles. There are no significant asymmetries in strength between right and left lower limb muscles
Sensory examination
Intact, there are no sensory disturbances.
Special test analysis:
- SLR- Negative
- Cross SLR- negative
- Slump-negative
Investigations:
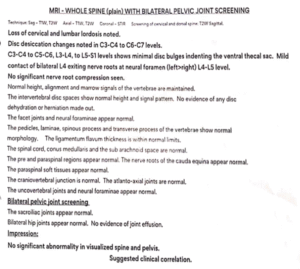
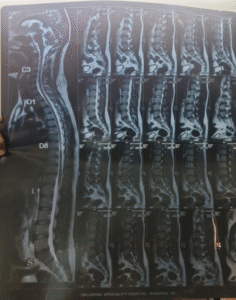
- MRI of the whole spine
- Normal. No abnormalities
- CT of the spine
- No abnormalities
- Blood test: Vitamin D and B12 deficiency were present. ESR, CRP – Normal
Differential diagnosis:
Lumbar radiculopathy
- No pain during coughing & sneeze
- No radiating pain, tingling/numbness sensation in the lower limb
- SLR, Cross SLR & slump are Negative, not reproducing pain
- No significant motor loss/ muscle weakness
Spinal Carcinoma
- There is no unexplained weight loss- He lost 12 kg in 6 months due to the siddha diet pattern only
- CT & MRI are normal
Ankylosing spondylitis
- No early morning stiffness for more than 30 minutes
- Pain is not relieved by movement & rest does not aggravate it
- MRI also normal – there are no impressions of sacroiliitis
- ESR and CRP are normal
Possible Diagnosis:
The possible diagnosis is Non-specific low back pain
Reasons:
- MRI and CT spine were normal, ruling out structural abnormalities. No red flag signs were present.
- Inflammatory blood markers were within normal limits, excluding systemic/infective/ inflammatory conditions.
- Radicular syndrome was clinically assessed and ruled out due to the absence of neurological deficits, dermatomal radiation, or nerve root involvement.
So, the low back pain contributing factors for this patient include sedentary lifestyle, reduced physical activity, previous pain experience, fear-avoidant behaviour, negative pain beliefs, unsuccessful prior treatments, Vitamin D and B12 deficiency. Hence, the presentation was categorised as Non-Specific Low Back Pain.
Treatment Planning:
1. Patient’s Belief and Expectations
The patient’s primary expectation is to return to normal life without pain
2. Overall Treatment Strategy
Since it is non-specific low back pain and the patient is physically inactive, it generally requires 15 to 20 sessions (8weeks)
- Weeks 1-4: 3 sessions per week- 12 sessions
- Week 5 & 6: 2 sessions per week- 4 sessions
- Week 7 & 8: 1 session per week – 2 follow-up sessions
Key things to focus on during treatment
- Reduce pain sensitivity
- Restore functional capacity
- Improve sleep
- Address fear and negative beliefs
- Promote long-term self-management
Weeks 1–4 (Desensitisation & Capacity Foundation):
Focus: Restore confidence and movement tolerance.
- Education to reduce fear, improve confidence, and encourage movement.
- Diaphragmatic breathing exercises to reduce pain sensitivity and promote relaxation.
- Gentle, Spinal and hip mobility exercises to restore normal movements.
- Low-load strengthening of trunk and lower limb muscles.
- Gradual exposure to walking or cycling to rebuild activity tolerance and confidence.
- Guidance on correcting Vitamin B12 and Vitamin D deficiency to support recovery.
Week 5 & 6 plan (Progressive Capacity Building):
Focus: Improve work capacity and general fitness.
- Progressing the strengthening exercises according to his capacity by modifying the intensity, volume or frequency.
- Focusing on strengthening the upper body also.
- Encouraging cardio to improve general physical health and fitness.
- Focusing more on home programs to encourage self-management.
Week 7 & 8 plan (Self-Management & Load Optimization):
- Advising on preventing recurrence & self-management.
- Explained clearly regarding Load management – advised to listen to the body & progressively overload the exercises every time.
- Strength & conditioning guidance provided – about Proper workout plan & how to do progression and Regression & RPE scales to achieve a better outcome in strength and fitness.