
Case prepared by: Sam
Seeing Possibility Beyond Surgery: A Case of Lumbar Radiculopathy with Mild Retrolisthesis
Patient profile:
- Age/Gender: 40-year-old Male
- Occupation: Mill Worker
Chief Complaint:
Severe low back pain radiating down the right lower limb, significantly affecting walking, sleep, work, and daily activities.
History:
The patient presented with complaints of low back pain radiating to the right leg.
Before the onset of symptoms, he was physically active and regularly engaged in walking and exercise.
Initial Episode (2024)
The patient experienced his first episode of low back pain in 2024. An MRI revealed a disc bulge, and he was managed with pain medications, following which his symptoms improved.
Aggravation Phase (November 2025)
In November 2025, while lifting weights, he experienced another episode of low back pain.
Although the pain increased, it remained tolerable, allowing him to continue his routine work.
However, after lifting weights again approximately 15 days later, the symptoms worsened significantly. This time, the pain radiated through the entire right lower limb.
Progression (February 2026)
Due to persistent worsening symptoms, he underwent a repeat MRI in February 2026.
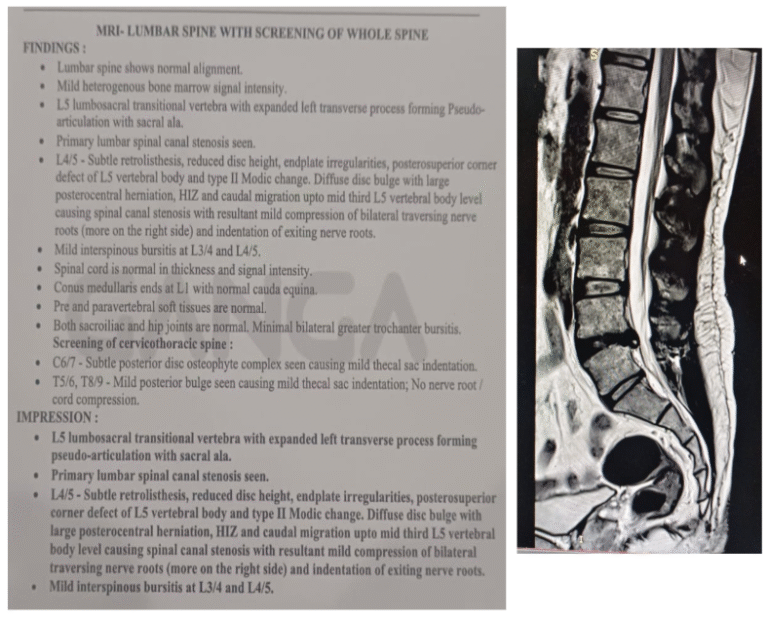
The MRI findings showed:
- L4–L5 disc herniation
- Mild retrolisthesis
Surgical intervention was suggested.
However, the patient was reluctant to undergo surgery and sought conservative management.
By this stage, he reported:
- Severe sleep disturbance due to pain
- Numbness in the right calf
- Inability to perform work-related tasks
- Reduced physical activity
- Significant movement-related fear
He consulted our clinic seeking recovery without surgery and aiming to return to normal daily life and work.
Past medical/surgical history:
No relevant past medical history
Lifestyle and Psychosocial factors analysis:
Physical activity status:
Poor. The patient was unable to engage in walking, exercise, or routine physical activity due to severe pain.
Sleep:
Severe disturbance due to pain
Stress:
High stress associated with the inability to work, exercise, and function independently due to pain.
Psychosocial factor
- Cognitive: The patient demonstrated good understanding and willingness to participate in rehabilitation.
- Affective: Emotionally distressed due to persistent pain and reduced independence.
- Social: Adequate social support.
Pain Analysis
Intensity: 10/10
Onset: Sudden
Location: Right buttock and calf > lower back
Duration: 15 days
Aggravating Factors: Standing, Walking, Lifting, Coughing, Sneezing
Relieving Factors: Pain medication
Lifestyle factor impact: Yes, the pain has significantly affected his sleep quality, physical activity, occupational performance, and emotional well-being.
Fear of movement analysis: Yes, movement-related fear was evident during standing, walking, and work-related physical tasks.
This suggested a significant protective behavioural response, likely contributing to reduced functional tolerance.
Our understanding of patient's problems:
The presentation suggested a radicular pain syndrome, but a thorough physical examination and investigations were required to confirm the specific type of radicular involvement, rule out other potential serious pathologies, and correlate MRI findings with clinically relevant symptoms.
Physical examination
Observation
No obvious postural or structural abnormalities.
Palpation
Tenderness noted over the right gluteal region.
Mobility screening
Forward Bending:
- Severely restricted due to pain.
- The patient could only reach up to knee level.
Squat:
- Normal and pain-free.
- This indicated preserved lower limb functional loading capacity.
ROM analysis
There is no restriction in hip, knee and ankle ROM on both sides.
Stability screening:
- The strength testing was not performed due to severe pain and irritability.
- However, during exercise trials, a greater motor control deficit was evident in the right lower limb
- This suggested reduced neuromuscular control secondary to pain inhibition.
Sensory examination:
Sensation was generally intact. However, the patient reported subjective numbness in the right calf region.
Special test analysis:
Slump Test: Positive on the right
Single Leg Raise: Positive on the right
Crossed Straight Leg Raise: Negative
These findings supported the concept of lumbosacral nerve root mechanosensitivity.
Investigation:
MRI (Feb – 2026)
Differential diagnosis:
1.Lumbar canal stenosis:-
Typically presents with:
- Bilateral symptoms
- Pain relieved by lumbar flexion
- Symptoms aggravated by extension
Why It Was Ruled Out
This patient demonstrated:
- Unilateral symptoms
- Pain aggravated during flexion
- No symptom provocation with extension
These findings were inconsistent with lumbar canal stenosis.
2. Retrolisthesis
Although MRI showed retrolisthesis, it was:
- Mild
- Subtle
- Clinically insignificant
Significant symptomatic retrolisthesis often presents with greater mechanical instability and broader symptom distribution.
The absence of traumatic history and predominantly unilateral radicular symptoms made it unlikely to be the primary pain source.
This highlights an important clinical principle: Not every MRI finding is clinically meaningful.
Possible Diagnosis:
Right lumbar radiculopathy
Reasons :
- Presence of unilateral radiating pain from the lower back to the right lower limb.
- Forward bending movements, coughing, and sneezing aggravate the pain.
- Leg pain is more than back pain.
- Sensory disturbances – numbness is present in the right calf area
- All the Neurodynamic tests are positive for lumbo-sacral nerve root involvement.
- MRI also confirmed the disc herniation with right nerve root compression.
- Other differential diagnoses were properly evaluated and ruled out.
Treatment Planning:
According to the severity of the pain, we planned for 20 sessions over a period of 8 weeks.
Week 1 & 2 : 3 sessions/ week – 6 sessions
Week 3 to 6: 3 sessions/ week – 12 sessions
Week-7 & 8: 2 sessions/ week – 4 sessions
Key things to focus:-
- Desensitise the Pain
- Improving neural mobility
- Improve the strength of the lower limb muscles
- Restoring his daily activities and preparing him for long-term self-management
Week 1 & 2 :- Pain modification and restoring confidence
- Educate the patient about pain to reduce his fear
- Diaphragmatic breathing for relaxation and pain modulation
- Neural gliding techniques within the symptom-tolerable level to improve neural mobility
- Gentle spinal and lower limb mobility exercises
- Isometric exercises for core, trunk and lower limb muscles
Week 3 to 6: Improving strength and functional restoration
- Focus on improving the strength of the lower limb muscles
- Gradual progression of load, reps completely based on response to symptoms
- Training functional activities relevant to his daily life and work demands
- Encourage walking and graded exposure to cardio exercises to improve cardio-respiratory fitness.
Weeks 7 & 8: Long-term self-management
- Advising on preventing recurrence and self-management.
- Explain clearly about load management -advice to listen to the body & progressively overload the exercises
- Strength and conditioning guidance provided- about a proper exercise plan, how to progress and regress the exercises and RPE scales to achieve a better outcome in strength and fitness.
Clinical Takeaway
This case demonstrates a vital lesson:
MRI findings alone should never dictate treatment decisions.
Although surgery was advised based on imaging, clinical assessment revealed that the patient’s presentation was consistent with a manageable lumbar radiculopathy responsive to structured rehabilitation.
A careful combination of:
- Clinical reasoning
- Progressive loading
- Patient education
- Functional restoration can often create meaningful recovery pathways without surgery.