IS EVERY RADIATING PAIN A SCIATICA?
A Clinical Case That Challenges MRI-Driven Labels
Low back pain radiating to the leg is often quickly labelled as sciatica, especially when an MRI report mentions a disc bulge. But is every radiating pain truly sciatica or radiculopathy?
This case highlights why clinical reasoning must always outweigh approaching a problem with imaging alone, and how fear-based interpretations can sometimes do more harm than the pathology itself.
Patient Profile
- Age/Gender: 27‑year‑old female
- Occupation: Fashion designer (Aari work – prolonged sitting at sewing machine)
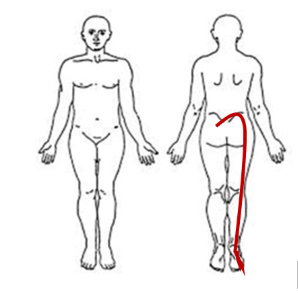
- Primary Complaint: Low back pain with radiation to the lateral thigh, leg, and foot on the right side
- Duration: Intermittent symptoms for 3 years, acute exacerbation over the past 3 weeks
History
In March 2022, the patient experienced low back pain radiating to the little toe. An MRI at that time revealed an L5–S1 disc extrusion, and she was diagnosed with sciatica. Management included a prolonged course of steroids, bed rest, avoidance of travel, and strict advice to stop gym activities—especially strength training and cardio—to prevent recurrence.
Following this advice, she:
- Avoided all exercises for 6 months
- Stopped consuming non‑vegetarian food for 15 months due to fear that it caused her condition
- Gradually developed a fear of movement and dependency on others
Over the last three weeks, she reported worsening pain with radiation down the right leg, which led her to seek further evaluation.
Current Functional Status
- Physical activity: No workouts for the past 6 months (previously underwent regular cardio, minimal strength training)
- Work tolerance: Unable to sit continuously for 4 hours
- Sleep: 7–8 hours, unaffected
- Psychological stress: High, due to inability to work, drive, or remain independent.
Pain Analysis:
- Intensity: 4–5/10 (moderate)
- Aggravating factors: Coughing, sneezing, walking >10 minutes, running
- Relieving factors: Rest
- Location: Lumbar region → right buttock → lateral thigh → leg → foot
- Irritability: Low–moderate (symptoms increase after ~10 minutes of walking)
- Sensitivity: High (pain takes time to settle once aggravated)
- Lifestyle impact: High impact to the extent that she quit her job.
- Fear of Movement: Present. Because the doctor advised her to stop moving. She believes that moving would worsen her problem.
Notably, the patient strongly associated movement with harm, reinforcing pain persistence. (But during the consultation with us, she did the movement after our encouragement and education towards movements)
Understanding the Patient’s Problem Based on History and Pain Analysis:
After visiting the doctor, the patient’s perception of pain underwent a significant change. She began to believe that she had sciatica caused by a disc bulge, which led her to stop moving her spine. She got pain after 10-15 minutes of walking. So, further we need to confirm whether it is radiculopathy or other potential differential diagnoses with proper physical examination and investigations.
Physical Examination
Observation
No visible postural or structural abnormalities
Range of Motion & Functional Tests
- Hip external rotation: Significantly reduced on the right side
- Forward bending: Reached mid‑shin
- Overhead squat: Full depth achieved, with a weight shift towards the left.
Strength Assessment (Key Findings)
| Strength test | Right | Left | Percentage |
|---|---|---|---|
| Single-leg sit-to-stand | 21 | 20 | 105% |
| Single hamstring bridge | 15 | 17 | 88% |
| Side plank leg lift hold | 17 | 38 | 44% |
| Single-leg calf raise | 25 | 26 | 96% |
| Single shin raise | 22 | 20 | 110% |
- Marked asymmetry in side plank leg lift hold (muscle weakness on the right side)
- No significant deficits in other lower‑limb strength tests
Neurological examination:
- Intact sensation; no dermatomal sensory loss
- Importantly, there was no motor loss or sensory deficit, significantly reducing the likelihood of radiculopathy.
Special Tests
- SLR / Cross SLR: Negative
- Slump test: Negative
- SI joint cluster: Negative
Psychosocial Contributors
- Cognitive: affected as she has catastrophic beliefs linked to MRI findings and prior medical advice
- Social: Affected- she withdrew from work and lost her independence
- Affective: Affected with emotional distress and fear of movement
Fear‑avoidance and prolonged inactivity likely amplified pain sensitivity and functional decline.
Investigations:
MRI (2022): L5 – S1 disc is desiccated and shows focal extrusion in the right para-central region, causing severe narrowing of the right recess and severe impingement of the right traversing S1 nerve root.
X‑ray spine: Normal
Blood reports:
- Haemoglobin: 10.2 g/dL
- Vitamin D3: 25 ng/dL
- Vitamin B12: <200 pg/mL (on supplementation)
Differential diagnosis:
Vitamin B12 deficiency:
- Yes, it’s present, but that alone isn’t the sole cause. She has also been avoiding non-vegetarian food for the past 15 months, which likely contributed to the vitamin B12 deficiency.
- Typically, B12 deficiency causes a burning sensation in the hands, feet, and upper trunk, but in her case, the burning sensation is confined to the lower limbs.
Lumbar radiculopathy
- There is no sensory and motor involvement.
- SLR /CSLR/ slump tests are all negative.
- The predicted probability for Lumbar radiculopathy is only 50 – 60% based on a clinical assessment scoring tool of sciatica.
Lumbar canal stenosis :
- There are no bilateral neurological symptoms,
- Extension of the trunk does not aggravate the pain and
- Also, in the MRI findings, there is no feature of it.
Diagnosis:
Lumbar radicular pain (L5–S1), without radiculopathy
Rationale:
- The patient presents with unilateral leg pain in an L5–S1 dermatomal distribution, aggravated by coughing and sneezing.
- Although MRI shows a prior L5–S1 disc extrusion, neurological examination reveals intact motor and sensory function with negative neurodynamic tests, indicating radicular pain rather than radiculopathy.
- Psychosocial factors and fear-avoidant behaviours appear to contribute to symptom persistence.
Treatment plan:
- Every patient is different! Some patients show sudden improvement, while others take time.
- Treatment duration: approximately 5 weeks – 3 sessions per week
Patient’s Goal:
- Go back to her work and self-travelling.
- She wants to do workouts in the gym.
Things need to be focused:
- Educating about her condition is important,
- Improve her tolerance & capacity.
- Strengthen the muscles of the lower limb and improve the hip mobility and overhead mobility.
- Graded exposure to activity is the goal.
Structured Treatment plan:
Week 1 :
- Educating about her condition and also focused on eliminating the negative beliefs towards her condition and MRI, and also how exercise will help for this condition.
- Nutritional advice is given because of the deficiency of haemoglobin, vitamin B12, and vitamin D3.
- Most importantly, provided the breathing exercises.
- Then concentrate on stretching the lower limb muscles to improve mobility in the lower back and hip.
Week 2 and 3
- Progressive strength training of lower limb & trunk muscles.
- Focus on restoring load tolerance and confidence
Weeks 4 and 5 and thereafter:
- Improving the steps count, walking time, and distance.
- Explained to her how hydration and sleep influence the pain.
- Her goal is to start gym activities. So explained clearly regarding Load management – advised to listen to the body & progressively overload the exercises every time.
- Strength & conditioning guidance provided, regarding:
- Proper workout plan
- How to do Progression and Regression
- Using RPE scales to achieve a better outcome in strength and fitness.
Key Takeaways for Clinicians
- Not all radiating pain is sciatica or radiculopathy.
- MRI findings must always be correlated with clinical examination.
- Absence of neurological deficit significantly alters diagnosis and prognosis.
- Fear‑based advice can perpetuate pain and disability.
- Education and graded movement exposure are powerful therapeutic tools.
Conclusion
This case reinforces the importance of thinking beyond imaging, recognising the role of psychosocial factors, and restoring patient confidence through movement. Radiating pain does not always indicate nerve damage. When clinicians address fear alongside physical capacity, outcomes can change dramatically.
Clinical reasoning, not MRI labels, should guide management.