
Case prepared by: Malathi
Seeing Beyond the X-ray: A Case of Load Intolerance knee pain
Patient profile:
- Age/Gender: 28 years, Female
- Occupation: Dentist
Chief Complaint:
Right-sided knee pain for 4 months, predominantly over the medial aspect, affecting occupational and daily activities.
History:
The patient complains of a 4-month history of right-sided knee pain, especially on the medial side. It made it difficult for her to sit in the dental chair and undergo the procedures. She visited an orthopaedic specialist, who said her back is weak, which is causing her knee pain and had her take an X-ray of her spine, which showed mild intervertebral space reduction. So, the orthopedician advised her to take painkillers and IFT to the lower back for 3 days, after which the back pain aggravated.
She consulted another orthopedician and took an X-ray of the right knee, which showed a reduction in the medial joint space. The doctor explained to her that her cartilage wore off due to poor nutrition during her pregnancy. This made her worry about her condition. So, she visited us seeking clarity, pain relief, and to get fit and strong.
Past medical/surgical history:
She underwent a C-section delivery 4 years ago, after which the back pain was intermittent.
Lifestyle and psychosocial factor analysis:
Physical activity status:
Poor physical activity. Although she occasionally participates in workouts and online fitness programs, she is not consistent.
Sleep:
She usually has a good sleep of about 7-8 hours on average.
Stress:
She reports moderate stress, worrying that experiencing pain at a young age may limit her ability to perform daily activities, occupational and family duties and could affect her mobility in the future.
Psychosocial factor analysis:
Cognitive: She had some negative beliefs regarding her pain and structural damage in her knee and back. She thinks that structural damage can worsen over time and is the reason for her not being able to have a normal life.
Affective: She is slightly affected as she worries that her pain will hinder her lifestyle.
Social: Good. Her family is supportive and helps her manage the pain.
Pain Analysis:

Intensity: 7/10
Onset: Gradual onset
Aggravating factor: Prolonged sitting with knees bent (common during dental procedures), standing on toes, cross-legged sitting for a long period, and standing for a long time
Relieving factor: rest
Location: Right knee, especially the medial side
Duration: 4 months
Lifestyle factor impact: moderate impact, as she had to modify several household and occupational activities because of pain.
Fear of movement analysis: She has a fear of hurting her knee while performing activities in the kneeling position. She performs the exercises, yet she’s a little concerned that it might hurt.
Our understanding of patients’ problems:
Considering her poor physical activity status and other features like pain aggravation with increased activity and pain reduction at rest, we suspect that the pain can be due to load-related mechanical pain. However, the medial joint space reduction, as in the knee, as she mentioned, is an uncommon finding for her age. Further physical examination and analysis of investigations are required to rule out any structural pathology, as in early-onset knee osteoarthritis.
Physical examination
Observational findings
Nil significant
Palpation:
No pain on palpation
Mobility screening:
Overhead squat: Good, slight discomfort in the anterior aspect of the knee in the deep squat.
Forward bending: Poor
ROM analysis
Knee flexion and extension: Full ROM
Ankle dorsiflexion: Mild reduction on the right side.
Hip external rotation: Reduced on the Right side
Stability screening:
Break test: Right side Hip abductors are weak and pain-free (significant weakness)
Investication:
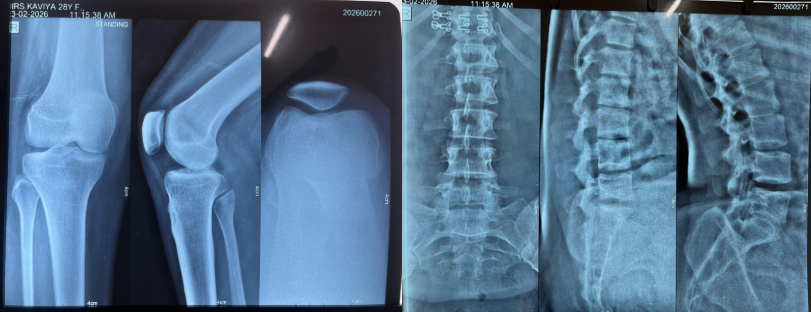
X-Ray:
In the knee X-ray, it appears to have an excessive medial joint space reduction in the A-P view; however, in the lateral view, the joint space is preserved. So it could be a technical error, like a misaligned beam angle, leg positioning error (not fully extending the knee, or a rotated leg while standing), which could give a fuzzy joint line, overlap of joint surfaces, and look blurred and narrow.
So this needs clinical correlation with the presenting symptoms.
Differential diagnosis:
Early Medial Compartment Knee Osteoarthritis:
Ruled out because:
- Younger age
- No previous history of injury to the knee
- No morning stiffness, swelling
- No progressive worsening
- No crepitus
- In X-ray, no significant joint space reduction, osteophytes, or subchondral sclerosis.
Medial Meniscus Irritation
Ruled out because:
- No trauma
- No locking or catching
- No joint line tenderness
- No swelling
Pain due to Lumbar Spine or back issue:
The doctor suspected this. Yet it is ruled out because:
- Pain aggravation is related to knee activity
- No neurological symptoms
- Back pain is not a primary complaint
Pes Anserine Irritation
Rule out because:
- No tenderness on palpation
- No localised pain specific to the pes anserine
Chondromalacia patella:
Ruled out because:
- No crepitus
- No pain with patellar compression
- No Retro-patellar pain
Possible Diagnosis:
Non-specific knee pain due to load intolerance
Validation:
- Pain aggravation with loading
- Pain relief with rest
- No consistent symptoms relating to structural damage
- Poor physical activity status
- Occupational demand for maintaining a particular position for a long time can aggravate the symptoms
- Deconditioning and reduced capacity due to a sedentary lifestyle.
- Right side lateral hip stability was reduced, which leads to right medial side knee pain.
Treatment Planning:
1. Patient’s beliefs and expectations
She has a lot of beliefs that she has structural damage in her knee and back, which has been confirmed by a few doctors, based on her X-rays. She expects to get
- Clear explanation of her condition
- Pain relief
- Return to normal daily, occupational, and functional activities
- Guidance on safe exercise to achieve good physical fitness
2. Overall Treatment Strategy
Goal:
- Eliminating negative beliefs
- Improving activity tolerance
- Improving Muscular Strength
- Encourage exercise adherence long-term.
3. Session planning:
We have planned a 10-session rehabilitation program.
Week 1 & 2: 3 days/ week – 6 sessions
Week 3 & 4: 2 days/ week – 4 sessions
Treatment:
Week 1: (Education & baseline strength)
- Educate that tissue damage is not equal to pain
- Patient education to eliminate fear related to activity
- Gradual exposure to low-intensity strength training and improved general overall lower limb mobility.
Week 2: (Improve adherence & Progressive Capacity Building)
- Progress the strength training as tolerated
- Address the ankle mobility restriction and Hip abductor weakness
- Include a goal-based rehab program- simple, achievable
- Introduce walking to improve cardiovascular fitness training
Week 3 & 4: (Load Optimization & Self-Management)
- Progressive strength training
- Improved cardiorespiratory fitness program
- Provide a structured exercise plan for better conditioning
- Explained clearly regarding Load management – advised to listen to the body & progressively overload the exercises every time.
- Guidance to continued strength training, cardiorespiratory training and lifestyle modification.