Diagnosis Lumbar Radiculopathy : A Case Study with Clinical Reasoning
Low back pain is one of the most common musculoskeletal complaints, but it is multifactorial. One of the important causes of low back pain is lumbar radiculopathy. However, differentiating it from other causes of back and leg pain requires careful clinical reasoning.
This case highlights how a structured assessment, integrating history, physical examination, psychosocial screening, and investigations, can lead to an accurate diagnosis and effective rehabilitation plan.
Patient Profile
- Age and gender: 25-year-old male
- Occupation: Unemployed
- Complaint: Left‑sided low back pain radiating to the left lower limb for 1 year.
History
One year ago, the patient was working in the construction field, which involved repetitive heavy lifting, inadequate rest, and poor recovery. Over time, he gradually developed low back pain. As symptoms persisted, he consulted an orthopaedic specialist and underwent MRI evaluation, which revealed a central posterior disc protrusion at L4–L5.
He was informed that surgical intervention might be required, which triggered significant fear and anxiety about his condition and future. Subsequently, he received physiotherapy treatment (IFT, traction, and stretching) for approximately six months. During this period, he was advised to use a lumbosacral belt lifelong and was repeatedly told that surgery would eventually be necessary. These messages reinforced fear-avoidance beliefs and movement avoidance behaviours.
Over time, his symptoms worsened, particularly in the early morning, and activities such as coughing and sneezing began to aggravate his pain significantly. Concerned by the progression of symptoms, he presented to our clinic for further evaluation and management.
Past medical/surgical history:
No relevant medical history related to the current complaints
Lifestyle And Psychosocial Context
Lifestyle:
- Physical activity: Very poor (sedentary lifestyle)
- Sleep: Disturbed due to pain and future‑related worries
- Stress: High, related to unemployment and persistent pain
Psychosocial Factors:
- Cognitive: Strong negative beliefs about pain and spine health influenced by repeated messages from healthcare providers, related to poor prognosis and surgery.
- Affective: Emotional distress, fear, and worry related to pain and unemployment.
- Social: Financial stress and limited support from family, as the patient is a single-parent child.
- These factors were considered critical, as they significantly influenced pain perception, disability, and recovery potential.
Pain Analysis:
- Intensity: 8/10
- Onset: Gradual
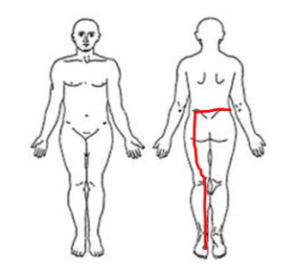
- Location: Left lower back, buttocks, posterior thigh, shin, and great toe
- Duration: 1 year
- Aggravating factors: Forward bending, lifting any weight, prolonged sitting, coughing, sneezing, and early morning (10–15 minutes)
- Relieving factors: Walking, gentle exercise, and rest
- Lifestyle impact: High impact, as he avoided most of the daily physical activities.
- Fear of movement analysis: Doctor/therapist induced, Pain & movement-related fear are present
Initial Clinical Impression
The unilateral radiating leg pain, dermatomal distribution, and symptom aggravation with coughing and sneezing raised a strong suspicion of lumbo‑sacral nerve root involvement.
Based on history and pain analysis, lumbar radicular syndrome was suspected. However, given the presence of psychosocial distress and short‑lasting early morning stiffness, a thorough physical examination was required to rule out other possible pathologies and confirm the diagnosis.
Physical Examination
Observation
Noticeable reduction in muscle mass on the left side involving the glutes, hamstrings, quadriceps, and calf muscles.
Palpation: Nil
Range of Motion (ROM) analysis:
- Reduced left hip internal and external rotation
- Forward bending caused spontaneous left knee flexion with severe back pain radiating to the leg.
Strength and Stability Screening
Significant weakness of the entire left lower limb was noted during isometric break testing (side‑lying hip abduction, prone knee flexion and extension)
The unilateral muscle atrophy and weakness were interpreted as a result of chronic neural compromise combined with disuse and fear‑avoidance–driven inactivity, rather than isolated mechanical pain.
Sensory examination :
Light touch and pressure sensations were largely intact; However, the patient reported intermittent subjective numbness over the left shin and great toe, which were consistent with L5 dermatome involvement.
Our understanding – Severe back pain and restriction of forward flexion and hip mobility with associated left-sided radiating pain strongly suggest lumbo-sacral nerve root involvement. The presence of left lower limb muscle weakness further supports the possibility of neurological compromise rather than isolated musculoskeletal pain. Yet, further assessments are required for confirmation.
Neurodynamic Tests
- Straight Leg Raise (SLR): Positive on the left side
- Crossed SLR: Positive on the right side
- Slump Test: Positive on the left side
Positive neurodynamic tests further supported lumbosacral nerve root irritation.
Investigations:
- MRI: Central disc protrusion at L4–L5 causing left neural foraminal narrowing & nerve root compression
- Inflammatory markers (ESR, CRP): Within normal limits
Differential diagnosis:
Ankylosis spondylitis
- ESR and CRP values are normal.
- Pain is not located in the SI joint.
- There is no early morning stiffness more than 30mins.
- There is no impression of Sacroilitis in MRI
Lumbar canal stenosis
- In stenosis, the entire spinal cord is getting compressed, so bilateral neurological symptoms will be present.
- But the person is having unilateral radiating pain. So we can rule out this
Spondylolisthesis of the lumbar vertebrae
- There is no history of trauma, lumbar extension is not painful and also there is no impression of listhesis on MRI.
Diagnosis:
The possible diagnosis is Left-sided Lumbar Radiculopathy
Validation:
- Presence of unilateral radiating pain from the lower back to the left lower limb.
- Forward bending movements, coughing, and sneezing aggravate the pain, and it is radiating to the left buttock, posterior thigh, shin and great toe.
- Leg pain is more than back pain.
- Significant motor loss (muscle weakness) is present in the left leg.
- Sensory disturbances – numbness is present in the left shin & great toe.
- All the Neurodynamic tests are positive for lumbo-sacral nerve root involvement.
- MRI also confirmed the disc protrusion with left nerve root compression.
- Other differential diagnoses were properly evaluated and ruled out.
Treatment Planning:
1. Patient’s Belief and Expectations
The patient’s primary goal was to return to daily activities and work without provoking symptoms.
2. Overall Treatment Strategy
Given the presence of lumbar radiculopathy with motor and sensory involvement, a minimum 3‑month rehabilitation program was planned, consisting of 24 physiotherapy sessions:
- Month 1: 3 sessions/week (12 sessions)
- Month 2: 2 sessions/week (8 sessions)
- Month 3: 1 session/week (4 sessions)
3. Key Things to Focus on During Treatment
- Reducing fear-avoidance, back & leg pain and the radicular symptoms
- Improving his overall joint mobility, strength of lower limb muscles and enhancing neural mobility
- Restoring his daily life activities & preparing the patient for long-term self-management
Month 1: Symptom Modulation and Confidence Building
- Pain neuroscience–based patient education to reduce fear
- Diaphragmatic breathing for relaxation and pain modulation
- Neural gliding exercises within symptom‑tolerable limits
- Gentle spinal and lower‑limb mobility exercises
- Pain‑free isometric activation of trunk and lower‑limb muscles, progressing to light isotonic work
Month 2: Strength and Functional Restoration
- Progressive strengthening (squats, lunges, hip hinge patterns), starting with body weight
- Gradual progression of load, repetitions, and complexity based on symptom response
- Training functional activities relevant to daily life and work demands
Month 3: Long‑Term Self‑Management
- Education on recurrence prevention
- Load‑management strategies and graded exposure to activity
- Strength and conditioning guidance, including exercise progression/regression and RPE‑based loading
Key Learning Points from This Case
- Lumbar radiculopathy diagnosis should be clinically driven, not imaging‑led.
- Fear‑inducing messages can significantly worsen pain and disability
- Unilateral weakness and positive neurodynamic tests strongly indicate neural involvement
- Active, graded rehabilitation with education is central to recovery
- Integrating biomechanics, neurodynamics, and psychosocial factors leads to accurate diagnosis and effective management of lumbar radiculopathy.