
Case prepared by: Nivetha
DON’T FEAR THE PAIN: UNDERSTANDING NON-SPECIFIC LOW BACK PAIN BEYOND MRI FINDINGS
PATIENT PROFILE
Age/Gender: 43-year-old Female
Occupation: Homemaker
CHIEF COMPLAINT:
Persistent bilateral lower back pain affecting daily activities and sleep quality.
HISTORY :
The patient reported that her back pain initially began in 2021 with severe intensity, to the extent that she was unable to comfortably perform basic activities such as going to the restroom.
At the onset of symptoms, she consulted a physiotherapist and underwent lumbar traction and IFT, but experienced minimal relief.
She later consulted an orthopedician and underwent an MRI, which revealed an L4–L5 disc bulge. Following this finding, she was advised to avoid: Forward bending, Lifting heavy objects, Physical exertion
Over time, this advice led her to adopt a completely sedentary lifestyle.
Although she intermittently used painkillers, the pain persisted and often worsened, especially:
- After attending social functions involving prolonged standing/sitting
- During periods of fasting
- During episodes of poor sleep
She also reported:
- More pain left side glute region
- Burning sensation in both feet
- Left heel and Achilles region discomfort
- Chronic insomnia
Despite trying multiple treatment approaches, her symptoms continued to recur and affect her daily life, sleep quality, and confidence in movement. That is the reason why she came to us seeking a better understanding of her pain and a long-term solution.
LIFESTYLE FACTORS AND PSYCHOSOCIAL ANALYSIS
Physical Activity
Completely sedentary after being advised to avoid bending and lifting following the MRI findings.
Sleep
Poor sleep quality with an average of 5–6 hours per night.
Stress
Increased stress levels secondary to chronic insomnia and persistent pain.
PSYCHOSOCIAL FACTORS
Cognitive
Mildly affected due to beliefs surrounding the disc bulge and fear of worsening the condition.
Affective
Moderately affected due to poor sleep quality and persistent pain.
Social
Affected by the physical demands associated with living in a joint family and managing household responsibilities.
PAIN ANALYSIS:
Pain Intensity: 9/10
Location: Bilateral lower back and more pain in the left side glute region
Duration: Since 2021, but currently Severe episodes lasting up to 2 months
Aggravating Factors: Prolonged sitting, Prolonged standing, Fasting periods
Relieving Factors: Rest, Pain medication
Lifestyle impact: yes, because she can’t sleep well.
Fear of movement analysis: not affected
Understanding the patient‘s problem, based on history and pain Analysis:
The patient’s history revealed something important:
Her pain consistently worsened after prolonged loading situations, such as attending social events involving extended standing or sitting. This suggested that the symptoms were less likely due to structural nerve compression and more likely load-induced pain
However, we need further examination to attain a correct diagnosis.
PHYSICAL EXAMINATION:
Observational finding:
No visible changes like swelling, redness, bruising, muscle atrophy, or hypertrophy.
Range of motion ( ROM ) Analysis:
Hip ROM: Normal
Knee ROM: Normal
Mobility screening:
- Overhead squat: Good
- Forward flexion: forward flexion is Good
Strength test:
| Strength Test | Right | Left |
|---|---|---|
| 1. Gluteus Maximus | Strong | Weak (Pain-free) |
| 2. Hamstring | Strong | Strong |
| 3. Quadriceps | Strong | Strong |
| 4. Hip Flexor | Strong | Strong |
The reduced left gluteal strength may have contributed to reduced lumbopelvic load tolerance during prolonged activities.
Palpation: No
Special test:
- SLR: Negative
- Crossed SLR: Negative
- Slump Test: Positive
A positive slump in isolation, without neurological findings, does not confirm radiculopathy and may simply reflect neural mechanosensitivity.
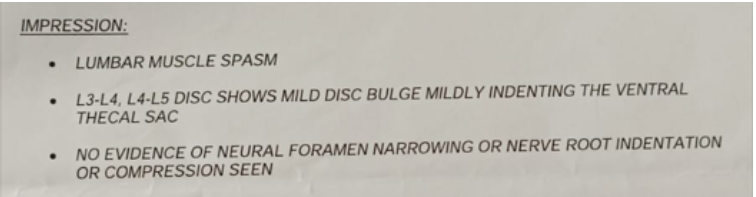
INVESTIGATION
- MRI taken 26 feb 2026 – L4-L5 disc bulge
DIFFERENTIAL DIAGNOSIS:
Sacroiliac Joint Dysfunction
Why It Was Considered Less Likely
- Pain was not localised to the SI joint belt region
- No characteristic SI joint referral pattern
- No associated morning stiffness
- Clinical findings were not suggestive of SI joint involvement
Lumbar Radiculopathy
Why It Was Considered Less Likely
- No neurological deficits
- Negative SLR
- Negative Crossed SLR
- No pain during coughing or sneezing
- No clear dermatomal symptom pattern
Although burning sensations were reported in both feet and the slump test was positive, the overall clinical presentation was not consistent with significant nerve root involvement.
Serious Spinal Pathology
Why It Was Considered Unlikely
No red flags were identified:
- No fracture history
- No infection
- No cauda equina symptoms
- No significant trauma
- No progressive neurological loss
DIAGNOSIS:
Patient's Perception of Pain
The patient believed that her MRI findings indicated ongoing damage and that bending or lifting could worsen her condition. This understanding contributed to movement avoidance and reduced physical activity.
Belief and expectations
She believes that a disc bulge means she should not bend forward, as it could lead to a disc prolapse
Possible Diagnosis:
NON-SPECIFIC LOW BACK PAIN
Contributing Factors
- Reduced Load Tolerance: Pain consistently increased after prolonged physical demand.
- Sedentary Lifestyle: Long-term movement avoidance reduces tissue capacity.
- Poor Sleep: Contributed to heightened pain sensitivity.
- Fear-Based Beliefs: The disc bulge was incorrectly interpreted as fragile.
- Stress: Likely amplified pain perception.
The Key Clinical Insight
This case highlights an important truth:
Pain does not always equal damage. An MRI finding like a disc bulge is common, even in pain-free individuals. The real issue here was not structural failure.
It was:
- Reduced physical resilience
- Lifestyle-related sensitization
- Misunderstanding of pain
TREATMENT PLANNING:
Primary Goal
Restore confidence, improve physical capacity, and help the patient return to a pain-free and active life.
Rehabilitation Duration
Approximately 8 weeks
Session Frequency
18 sessions total; Progression: 3 sessions/week → 2 sessions/week → 1 session/week
Things to focus on during Treatment
- First, focus on patient education ( because she wrong understanding of her condition )
- We need to guide how to improve a healthy lifestyle, also follow the sleep pattern, 4-5 litres of water intake and reduce stress.
- Improve her capacity to tolerate the pain.
- Teaching about load management.
- First, start GRADED EXPOSURE( rehab phase) and after we focus on TRAINING PHASE (strengthening exercises).
TREATMENT FOCUS:
Phase 1: Education & Reassurance
Helping the patient understand:
- A disc bulge does not mean damage progression
- Bending is safe
- Pain is modifiable
- Movement is medicine
Phase 2: Lifestyle Optimisation
Focus on:
- Sleep hygiene
- Stress management
- Regular hydration
- Daily movement exposure
(Water intake recommendations should be individualised rather than fixed at 4–5 litres.)
Phase 3: Graded Exposure
Gradual reintroduction to:
- Forward bending
- Functional loading
- Prolonged standing tolerance
- Daily activity demands
Phase 4: Strength & Capacity Building
Progressive strengthening:
- Core endurance
- Hip strength
- Functional lifting patterns
- Whole-body resilience training
CLINICAL TAKEAWAY
This case reminds us that successful rehabilitation often begins by changing beliefs, not just treating tissues.
Sometimes, the biggest barrier to recovery is not the disc itself. It is the fear attached to the diagnosis.
When we educate, reassure, and progressively reload the system, recovery becomes possible.