
Case prepared by: Surendar
Understanding and Managing Non-surgical SLAP tear in a professional cricketer
Patient Profile
- Age and gender: 26-year-old male
- Sport: Professional Cricket Bowler (bowling speed: 130 km/h)
- Complaint: Right shoulder pain, present for 1.5 years
History:
In June 2023, after an intense day of bowling, the athlete returned home and began experiencing pain in his right shoulder. He thought it was normal shoulder pain and that it would subside in a day or two, but the pain didn’t. He sought medical advice and was treated with a painkiller injection. There is no past medical or injury history.
As months passed, the pain did not resolve, so he took an MRI scan in November 2023. The results show a SLAP II Tear, and the doctor advised surgical intervention. However, he was not interested in surgery, and instead, he underwent a rehabilitation program under the guidance of his team physiotherapist and another physiotherapy clinic. It encompassed mobility and low-intensity strengthening. This protocol helped to relieve some pain and range of motion, but some pain persisted, especially at the end range of motion.
Two months ago (October 2024), with the advice of team physio, he progressed to gym-based strength training on his own. While his overall shoulder condition improved, he continued to experience pain at the end range of shoulder flexion. His primary goal now is to return to competitive bowling without pain or limitation. He consulted us for a return-to-sports program.
Physical activity status: Maintaining an active lifestyle, including strengthening exercises at the gym.
Sleep: He sleeps well, averaging 6-7 hours every day.
Stress: Doesn’t report any stress. But he has not played for a year and a half, which might stress him out.
Pain Analysis:
- Intensity: 2-3/10
- Aggravating Factors: End range shoulder flexion, sometimes during bowling
- Relieving Factors: Rest.
- Location: Area around the right shoulder, especially in the anterior aspect of the shoulder
- Duration: 1 and a half years
- Type of Pain: nociceptive pain
- Irritability: High
- Sensitivity: Low
- Lifestyle Impact: Minimal
- Fear of Movement Analysis: Initially, Pain-related fear of movement is present. At present, he has no fear of movement.
Understanding the Patient’s Problem Based on History and Pain Analysis:
- As an overhead athlete with repetitive high-velocity bowling, SLAP tears are common. However, some anatomical adaptations occurring in overhead athletes may resemble a SLAP tear in imaging. I suspect that his initial pain might have started due to improper load management because, during bowling, he didn’t have any pain. Only after reaching home he started feeling pain.
- So, need to rule out other potential differential diagnoses.
Physical Examination
- Observational Findings: No visible changes like swelling, redness, bruising, muscle atrophy, or hypertrophy.
- Range of Motion (ROM) Analysis:
- Total arc
- Right- 160º (IR-60º+ ER- 100º)
- Left- 170º (IR-95º + 75º)
- Mobility Screening:
Shoulder Overhead flexion mobility: Right side reduced
Stability Screening: Strength Test
| RIGHT | LEFT | Symmetrical index |
Shoulder External Rotation (ER) max rep 2kg | 24 | 20 | 120 % |
Chest-supported Rowing max rep 15kg | 19 | 20 | 95 % |
Kneeling Shoulder Press max rep 10kg | 19 | 19 | 100 % |
Single-arm DB press max rep 12.5kg | 26 | 32 | 81.25 % |
Biceps curl max rep 7.5kg | 10 | 12 | 83 % |
Triceps overhead extension max rep 5kg | 17 | 20 | 85 % |
- Palpation: No pain on palpation
Special Tests:
- O’Brien test: Negative
- Biceps load test I: Negative
- Biceps load test II: Negative
Return to sport testing:
After 4 weeks of rehabilitation, RTS testing was performed to acquire more information about the athlete’s current status.
TEST | RIGHT | LEFT | Symmetrical index |
Med ball Open Kinetic endurance test | 30 | 24 | 125 % |
Ball drop catch test | 41 | 37 | 110 % |
Single-arm Seated med ball throw | 9 ft 4in | 9 ft 9 in | 95 % |
CKCUES Test | 14 | 12 | 116 % |
Upper Limb Rotation Test | 16 | 15 | 106 % |
Investigation:
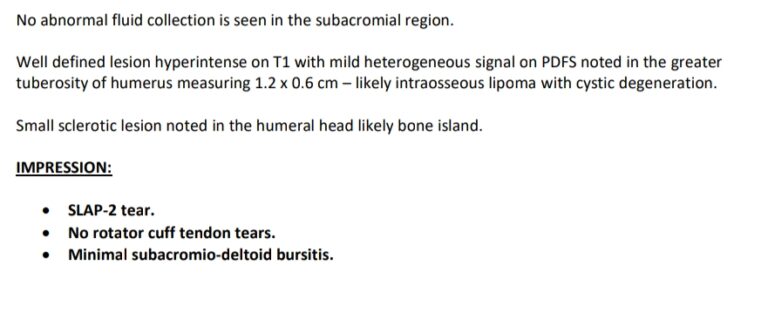
MRI (Nov 2023): SLAP II Tear
Differential Diagnosis
1. Rotator Cuff related shoulder pain
This is common in bowlers due to repetitive stress.
Rule Out:
- No weakness in external rotation
- Pain is not aggravated by resisted external rotation or pressing movements.
- MRI does not report rotator cuff pathology.
2. Biceps Tendinopathy
- Involvement in SLAP tears.
- Pain in the anterior shoulder.
Rule Out:
- No pain on palpation of the bicipital groove.
- No clear pattern of pain with resisted elbow flexion.
- All special tests are negative.
3. AC joint pathology
- No history of trauma or injury
- No difference in scapular positional changes
- Negative active compression and horizontal adduction test
Diagnosis:
- Suspected Slap 2 tear, which has healed or potentially improved within this 1.5years
- Doubted MRI predictability as well and suggested to repeat MRI
- Progressed for RTS
Validation for the diagnosis:
- Diagnosis: Post SLAP Type II Tear status
Validation:
- Being an overhead athlete who is involved in repetitive high-velocity sport (bowling-130 kmph) predisposes him to SLAP tear.
- He has GIRD (Glenohumeral Internal Rotation Deficit), which is a common adaptation seen in overhead athletes and serves as a risk factor for SLAP tear.
- Symptoms match with SLAP pathology, including:
- Pain with overhead movement (bowling)
- Had mobility restrictions at the onset of pain
- Gradual onset after high workload
- The MRI confirms a SLAP II tear
However, the O’Brien test, biceps load test I, and biceps load test II are negative. So either the SLAP tear is healed now, or the MRI report may be wrong (Normal adaptation in overhead athletes looks like SLAP tear in MRI).
Other factors to consider:
- Patient’s perception of pain: He has a good understanding of the pain and the importance of exercise. We need to give the right course of RTS rehab.
- Psychosocial Factor analysis: Not affected
- Belief and expectation: He believes that he can bowl the same as before if he undergoes a proper return to the sports program.
Treatment Planning
- How long it takes – Usually, non-surgical management of SLAP tear takes around 5-6 Months to return to play
- How many sessions are required – The average session required is 20 (18-28 sessions)
- How many days in a week – 2,2,2,1,1,1,1,0,1,0,1,0,1,0,1
- Things need to focus during treatment
1. Mobility exercises
- Shoulder overhead mobility like Foam Roller Lat stretch, sleeper stretch
- thoracic extension mobility like Foam roller thoracic extension, wall-supported thoracic exercise
- scapular mobility exercises like Wall angels, scapular pushups, Prone V, T, and A exercises
- Strength training for Upper body like Single arm DB chest press, kneeling shoulder press, Landmine Shoulder Press chest supported rowing, Lateral raises, biceps and triceps strengthening exercises
- Strength training for core muscles, like Banded rotation and lower body muscles
- Stability exercises like Turkish getup, Thread a needle
2. Power-based movements – to produce force development during bowling
- Explosive pushing and pulling like Pendlay rows, Push press, explosive Smith machine bench press
- Rotational power training like Woodchops, Med ball rotational throw, Med ball overhead rotational slam
- Upper body Plyometrics like plyo pushup, clapping pushup
Sports-specific conditioning- Bowling-specific movement like med ball overhead, bowling with a weighted ball in half kneeling, Bowling-Specific Resistance Band exercise.
Progressive bowling program (including workload tracking)
- Shadow bowling with low intensity
- Partial effort bowling (50-60%)
- Progress to full-effort bowling
- Return to competitive-level bowling