Understanding and Managing Shoulder Pain in a Recreational tennis player
Patient profile
- Age and Gender: 43-year-old male
- Occupation: IT worker
- Sport: Recreational Tennis Player and a triathlete; also plays cricket and badminton.
- Complaint: Right Shoulder pain for 2-3 years
Patient profile
- Age and Gender: 43-year-old male
- Occupation: IT worker
- Sport: Recreational Tennis Player and a triathlete; also plays cricket and badminton.
- Complaint: Right Shoulder pain for 2-3 years
History:
The pain began in 2022 while playing cricket, specifically during bowling, when he felt a pulling sensation in his shoulder. He immediately consulted a doctor and underwent an X-ray, which showed no abnormalities. Despite receiving treatment, it was ineffective. Following the onset of pain, he stopped playing both tennis and cricket and avoided exercise for about two months. When he tried playing tennis again, the pain returned, forcing him to play only occasionally while managing the discomfort.
Over time, he consulted multiple doctors and physiotherapists and underwent various treatments, including muscle relaxants, painkillers, ultrasound therapy, TENS, and basic exercises. However, his pain did not subside and has now persisted for 2-3 years. Now, he has consulted us to reduce his pain and return to sports without discomfort. There is no past medical or injury history.
Physical activity: He is maintaining an active lifestyle that includes stretching and strengthening exercises at 2-3 days a week at home and the gym, additionally, he goes for recreational runs.
Sleep: He sleeps well, averaging 6-7 hours every day.
Stress: He does not report stress. However, due to this persistent pain, there may be some mental stress.
Pain Analysis:
- Intensity: 2-3/10
- Aggravating Factors: Tennis swing movements (horizontal abduction, adduction, shoulder internal rotation), pouring water or tea into a cup, and lying on the affected shoulder.
- Relieving Factors: Rest, all activities other than aggravating factor.
- Location: Right side of the shoulder in the deltoid region above the deltoid tuberosity
- Duration: 2-3 years
- Type of Pain: Mixed
80% Nociceptive, 20% Nociplastic (the pain is influenced by doctor and internet-induced misbelief)
- Character: mechanical pain (Sharp pin-pricking in nature)
- Irritability: High
- Sensitivity: Low
- Lifestyle Impact: Moderate impact, he loves to play tennis, but due to pain, he could not play.
- Fear of Movement Analysis: Pain-related fear of movement is present.
Understanding the Patient’s Problem Based on History and Pain Analysis:
Suspecting an AC joint pathology, as he has pain during horizontal adduction. We need to rule out other possible diagnoses before confirming the diagnosis. He has a pain-related fear of movement – we need to work on patient education.
Physical Examination
Observational Findings: Right-side deltoid and arm appear hypertrophied compared to the left side. (It is common in tennis players, so no need to pathologize it)
- Range of Motion (ROM) Analysis: Shoulder external rotation ROM reduced on the Right side
- Mobility Screening:
Overhead flexion mobility: reduced on the Right side
Thoracic rotation: reduced on the Right side
- Stability Screening:
Isometric break test: Right-side shoulder external rotators are comparatively weak and pain-free.
- Palpation: No pain over the deltoid area or the AC joint
- Special Tests:
- Biceps load test 1 – negative
- Biceps load test 2 – negative
- O’Brien test (active compression test) – negative
- Strength Test
| Test | Right (Involved) | Left (Uninvolved) | Symmetrical Index |
|---|---|---|---|
| Shoulder External Rotation (ER) | 30 | 26 | 115% |
| Chest-Supported Rowing | 21 | 17 | 123% |
| Kneeling Shoulder Press | 10 | 10 | 100% |
| DB Bench Press | 10 | 11 | 91% |
| Upper Limb Rotation Test | 16 | 10 | 160% |
No significant deficits were observed in the strength test.
Investigation
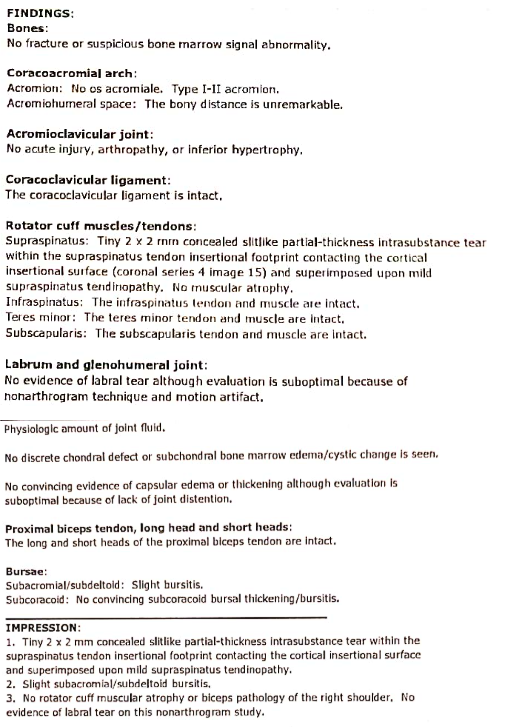
MRI taken 2 months back reveals a 2mm x 2mm insertional supraspinatus tear.
Differential Diagnosis:
1. Acromioclavicular (AC) Joint Pathology
Symptoms include pain localized to the AC joint, pain with horizontal adduction, and tenderness on palpation.
Ruling Out: In this case, there is no isolated AC joint tenderness, and the MRI did not indicate AC joint pathology. Pain is present in horizontal adduction but not on the AC joint. Pain is located in the mid-deltoid. Active compression test is negative; AC joint pathology is less likely to be a diagnosis.
2. SLAP Tear
Rule out: Biceps load test 1 and 2 are negative, O’Brien test (active compression test) is also negative. SLAP tear is ruled out as these 3 tests collectively have 99% sensitivity and specificity for SLAP tear. MRI doesn’t show any SLAP tear as well. So the likelihood of SLAP tear is lower.
3. Supraspinatus Tear
A partial-thickness tear of the supraspinatus can lead to pain and weakness, particularly during abduction and external rotation.
Ruling Out: While the MRI does show a small supraspinatus tear, the patient’s symptoms are not entirely consistent with an isolated supraspinatus tear. He does not exhibit significant weakness in abduction or external rotation, nor does he have localized tenderness at the supraspinatus insertion. Therefore, the tear may be incidental rather than the primary cause of pain.
Diagnosis:
Rotator cuff-related shoulder pain due to overuse of the shoulder comes under the strong, painful shoulder category.
Validation:
The diagnosis is confirmed as Rotator Cuff-Related Strong Painful Shoulder rather than Weak Painful Shoulder, as strength testing indicates that the painful side retains sufficient strength. Although the MRI reveals a supraspinatus tear, its clinical significance remains uncertain as it may not be the primary source of the patient’s shoulder pain. Additionally, being involved in overhead sports predisposes him to the RCRSP.
Other factors to consider:
- Patient’s Perception of Pain: The patient does not have a clear understanding of his pain, as he is confused about whether it will subside or not.
- Psychosocial Factor Analysis: The Cognitive factor is affected. His thoughts and beliefs about pain are not good.
- Belief and Expectations: He is very confused and scared about his pain because even after consulting many doctors and physios, he didn’t improve. The patient expects to achieve a pain-free life, and he believes that we can help him improve his condition.
- Impairment:The patient’s pain is most likely due to an impairment in force production and neuromuscular control rather than a specific structural pathology.
Treatment Plan
Things that need to be focused on during treatment:
- Patient Education
- Thoracic Rotation Mobility
- Shoulder Overhead Flexion Mobility
- Shoulder External Rotation Mobility
- Proper Muscle Strengthening and Activation in the shoulder and neck muscles.
- Power and Conditioning-Based Shoulder Exercises
- Core Strengthening
Treatment strategy
| Week | Things to be focused on | Exercises (Examples) |
|---|---|---|
| Week 1- 2 | Patient Education (Educate the patient about his condition, duration for recovery, and the rehab journey, as well as provide reassurance), Regaining ROM, activating the Shoulder muscles. | Banded Lat stretch, Downward facing dog alternate toe touch, Prone angels, Prone V and T, Dumbbell Shoulder external rotation, Shoulder wall clock, Scapular pushup. |
| Week 3-6 | Shoulder Strengthening | Bench press, Overhead press, Rowing, Lateral raise, Cuban Press, Facepull. |
| Week 7-8 | Power-based shoulder movement, Shoulder stability exercise | Landmine shoulder press, Pendlay rows, Smith machine bench press, Med ball chest pass, Med ball Overhead rotational slam, Turkish getup, windmill. |
| Week 9-12 | Sports-specific movement | Woodchops, Banded fly, Banded core rotation, Kneeling med ball rotational throw. |